9. PROCEDURES FOR INTERMITTENT CATHETERISATION
9.1 Choice of technique
The choice of technique depends on the setting where intermittent catheterisation (IC) takes place, who performs the catheterisation, and the local policy of the different countries (see Diagram 5). In hospital settings, there are rising concerns about infection control, indicating that sterile technique is needed. [24]
A small study (n=36) in spinal cord injury patients who were catheterised by a nurse specialist indicated that clean IC (in these guidelines described as a non-touch technique in the rehabilitation setting) did not place the [110] patients at increased risk for developing symptomatic UTI. [151] The evidence for clean technique is weak and due to the risk of cross-contamination. Catheterisation by a healthcare professional is always with a sterile (theatre) or aseptic technique (ward or community setting). The European Association of Urology guidelines on neurogenic bladder dysfunction state that an aseptic technique is the most appropriate compromise between UTI incidence, practicality and economic viability. [27]
For patients and caregivers in the community setting, clean/non-touch rather than aseptic IC is agreed to be a safe and effective procedure with no increased risk of symptomatic urinary tract infection (UTI).
Diagram 5. Intermittent catheterisation techniques – simplified
This diagram gives a simplified overview of the use of the different techniques in different settings, but is not meant to be prescriptive in any way.
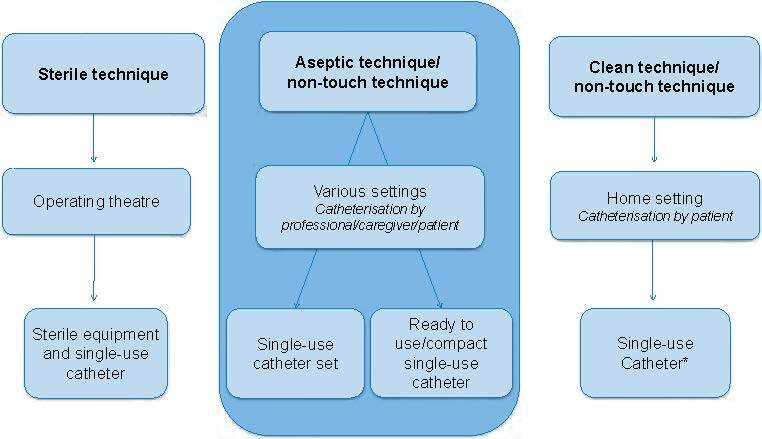
NB: If single-use catheters are not available, use reusable catheter
9.1.1 Intermittent catheterisation by healthcare professionals and patients/caregivers
For practical guidelines on how to insert a male or female urethral intermittent catheter, see Appendices B–E and G.
Procedures are listed in:
- Appendix B Male urethral catheterisation by a healthcare professional – Aseptic procedure
- Appendix C Female urethral catheterisation by a healthcare professional – Aseptic procedure
- Appendix D Male urethral catheterisation by a healthcare professional – Non-touch procedure
- Appendix E Female urethral catheterisation by a healthcare professional – Non-touch procedure
- Appendix G Patient/caregiver teaching procedure intermittent self-catheterisation - Female and male
| Recommendations for IC by a healthcare professional | LE | GR |
| Use local guidelines on procedure for IC [152] | 4 | C |
| Use a sterile single-use intermittent catheter to prevent cross-contamination in clinical, rehabilitation, and long-term care settings [24] | 1 | B |
| Check for allergies/sensitivity (e.g., lidocaine or chlorhexidine) if using a lubricant* [153, 154] | 4 | C |
| Do not use antiseptic lubricants for IC routinely* [153] | 4 | C |
* Recommendations with an asterisk (*) should be included in the patient/caregiver education on IC.
9.2 Choice of catheter and equipment
Catheter materials are described in Chapter 6. The choice of catheterisation equipment depends on the patient and/or caregiver assessment being undertaken and the patients’ preferences as described in Section 7.3. It is recommended that, when choosing a coated intermittent catheter, physicians and patients should not rule out pre-lubricated catheters for safety reasons alone. [54]. In case of incomplete bladder emptying, a micro-hole zone catheter may be useful. [155]
Catheter type and characteristics vary as do reasons why individuals need to perform IC. When choosing which product to use, consideration must be given to patient preference, limitations or disabilities, cost–benefit analysis, cost-effectiveness, ease of use, and storage. Patients may use multiple types of catheters/systems depending on their activity. Availability of different types of catheters differs among countries and patients need to check local reimbursement practices.
Lubrication or coated catheter
Hydrophilic-coated catheter
The risk of urethral trauma while introducing hydrophilic-coated catheters is diminished and there is evidence to suggest a lower incidence of catheter bypass and urethral irritation. [156] Bacteria can be introduced during catheter insertion as a result of trauma; hydrophilic coatings cause less trauma, and thus reduce the risk of complications in terms of haematuria and pain. [68, 157]
A systematic review of real-world data evaluated the incidence of UTI in patients using pre-lubricated versus hydrophilic catheters. Pre-lubricated catheters were associated with a significantly lower number of symptoms suggestive of UTI compared to the group using hydrophilic catheters. [54]
Various studies have shown discomfort on withdrawal of hydrophilic-coated catheters in patients who take a longer time to manage IC. [103, 123, 157, 158] Most of the available literature suggests that most patients prefer to use a coated single-use catheter for convenience, discretion, comfort, improved quality of life, and reduced episodes of UTI. [73, 123, 127, 159]
Non-coated catheters
Non-coated catheters require the use of lubricants. Female catheterisation has traditionally been performed using either no gel or a small amount of lubricant on the catheter tip. In both male and female patients, the vulnerable urothelium can only be protected by an unbroken film of lubricant. This implies that lubricants must be instilled into the urethra, and not on the catheter, or else the lubricant can be wiped off at the entrance to the urethra and, therefore, does not reach the narrow, more vulnerable parts. Lidocaine anaesthetic gel is recommended for men, although some women with urethral sensation may need to use it too. Anaesthetic gels are contra-indicated in patients with known allergies/sensitivity to the active ingredients, and those who have damaged/traumatised or bleeding urethral membranes, because there is an increased risk of systemic absorption of lidocaine hydrochloride. [153]
9.3 Meatal cleansing
Except for complete sterile technique in operating theatres (see Section 4.2), water and soap can be used for meatal cleansing (or only water if there is no evidence of soiling), because it has been shown that water is as safe as antiseptic for preparation of the meatus (men) or vulval area (women) before inserting a catheter. [154, 160-162] However, these studies were all carried out with indwelling catheters.
One study showed that use of chlorhexidine in meatal cleansing reduced catheter-associated UTI. [163]
| Recommendations | LE | GR |
| Clean the urethral meatus with water and pH-neutral soap [154, 160-162] | 1a | A |
| Use lubricants in both women and men when using a non-coated catheter [153] | 4 | C |
| Choose lubricant/type of catheter coating based on a comprehensive patient assessment and the reasons for IC | 4 | C |
| Choose a catheter size large enough to allow free drainage but small enough to reduce risk of trauma | 4 | C |
| Inform patients using reusable catheters how to handle the catheter with cleaning, storage and lubrication according to local guidelines [107] | 4 | C |